Main Menu
Main Menu |
|
Most Favorited Images |
|
Recently Uploaded Images |
|
Most Liked Images |
|
Top Reviewers |
| cockalatte |
645 |
| MoneyManMatt |
490 |
| Still Looking |
399 |
| samcruz |
398 |
| Jon Bon |
385 |
| Harley Diablo |
373 |
| honest_abe |
362 |
| DFW_Ladies_Man |
313 |
| Chung Tran |
288 |
| lupegarland |
287 |
| nicemusic |
285 |
| You&Me |
281 |
| Starscream66 |
264 |
| sharkman29 |
252 |
| George Spelvin |
248 |
|
|
Top Posters |
| DallasRain | 70426 | | biomed1 | 60651 | | Yssup Rider | 59981 | | gman44 | 52939 | | LexusLover | 51038 | | WTF | 48267 | | offshoredrilling | 47591 | | pyramider | 46370 | | bambino | 40333 | | CryptKicker | 37085 | | Mokoa | 36487 | | Chung Tran | 36100 | | Still Looking | 35944 | | The_Waco_Kid | 35414 | | Mojojo | 33117 |
|
|
 02-04-2012, 06:03 PM
02-04-2012, 06:03 PM
|
#196
|
|
Valued Poster
Join Date: Nov 7, 2010
Location: Top of The World
Posts: 601
|
Quote:
Originally Posted by Wakeuр

Bill...what's your point in posting all of this here on this website?
|
The HIV/AIDS scam is a great evil - perpetrated against a largely ignorant and naive public - millions have been killed - due to a faulty science based on fraud and greed.
I am but a small part of a growing awareness that's fighting back.
Join me - or succumb to those so-called symbols of authority who intend to take everything from you - a.k.a. your executioners.
.
|

|
 | 1 user liked this post |
|
02-04-2012, 06:22 PM
|
#197
|
|
Valued Poster
Join Date: Nov 7, 2010
Location: Top of The World
Posts: 601
|

The Padian Study – Sex is not the Problem
While these ‘researchers’ were watching, for six years of up, down, in and out sex, nobody managed to trick their surrogate marker assay (that’s “hiv test” in the press), from negative to positive. - “We followed up 175 HIV-discordant couples [one partner tests positive, one negative] over time, for a total of approximately 282 couple-years of follow up… No transmission [of HIV] occurred among the 25% of couples who did not use their condoms consistently, nor among the 47 couples who intermittently practiced unsafe sex during the entire duration of follow-up…”
- “We observed no seroconversions after entry into the study [nobody became HIV positive]…This evidence argues for low infectivity in the absence of either needle sharing and/or other cofactors.”
That is, these people were having sex with “positives” for six years, and managed not to become “positive” themselves.
Why the quotes around “positive?” Because the tests are actually more or less “reactive.”
“Positive” or “negative” is implied, (not inferred) later, on the basis of the perception of “risk” in the person being “tested.”
A lot of quotes, but there are so many undefined, overly-broad, and imprecise words used in AIDS-speak, it’s necessary to take a step back and understand what it is they’re actually talking about.
So, Padian. Zero seroconversions in 6 years of humping, (in every orifice, she records). But the reality is, that the tests are surrogate markers – stand-ins. They don’t record the presence of a specific particle anyway.
They grab a variety of proteins, with synthetic molecules that are manufactured these days, in bacteria, according to consensus agreements of how much they ‘should’ weigh.
The proteins have shown an affinity for just about any condition of illness, and even many non-illnesses. So, pregnant women, drug users, hemophiliacs, children, mice, dogs, goats and cows, all have proteins that trick the tests into being “reactive.”
“Positive” comes later, when you think you’re testing someone who is “at risk.”
It’s not science, but it’s popular, nonetheless.
The Padian Study: http://liamscheff.files.wordpress.co...-sex-study.pdf
.
|
|
|
| 1 user liked this post |
|
02-04-2012, 08:23 PM
|
#198
|
|
Valerie's Mod Husband
Join Date: Dec 13, 2010
Location: Houston
Posts: 28,030
|
Quote:
Originally Posted by Mr. Bill
The HIV/AIDS scam is a great evil - perpetrated against a largely ignorant and naive public - millions have been killed - due to a faulty science based on fraud and greed.
I am but a small part of a growing awareness that's fighting back.
Join me - or succumb to those so-called symbols of authority who intend to take everything from you - a.k.a. your executioners.
.
|
You didn't answer the question Bill. Why on this website?
|
|
|
| 1 user liked this post |
|
02-04-2012, 08:31 PM
|
#199
|
|
Valued Poster
Join Date: Nov 7, 2010
Location: Top of The World
Posts: 601
|
Quote:
Originally Posted by Wakeuр
You didn't answer the question Bill. Why on this website?
|
Why? ...because it appeared no one else had the essential competency, a selfless inclination, or the balls to speak up.
.
|
|
|
| 1 user liked this post |
|
02-04-2012, 10:59 PM
|
#200
|
|
Account Disabled
Join Date: Apr 25, 2011
Posts: 2,275
|
Bill, by your signature line, it is obvious you intend to make ECCIE the respository of your dissertation on this conspiracy theory. How many more "chapters" before you are conferred the PhD in Dipshitarianism?
To everyone else, there is ample reason to believe pharmaceutical companies are strictly money-grabbing entities dispensing dangerous chemicals for everything from invented disorders (such as describing a child who doesn't want to do their homework (DSM 315.4) or who argues with their parents (DSM 313.8)) to psycho-somatic symptoms better relieved by improved diet, vitamins, and exercise, however this diatribe dissertation makes Mr. Bill look like a total nutjob.
What may have proven interesting and may have generated a desire in many for more information through a well presented discussion in a couple of posts with links to research material, instead has turned into a mindless data dump reminiscent of one of my most thorough bowel cleansings.
Any traction he had at the beginning was long ago lost.
Now Mr. Bill appears simply to be a wacko and is actually destroying any chance for credibility.
But hey, 2012 has begun with a number of mental meltdowns on ECCIE, so what else is new?
|
|
|
| 1 user liked this post |
|
02-04-2012, 11:15 PM
|
#201
|
|
Valued Poster
Join Date: Nov 7, 2010
Location: Top of The World
Posts: 601
|
HAART Exposed: Sustiva Causes AIDS Symptoms
2 Sept 2010 – Last year, OMSJ identified the HIV drug Sustiva (Efavirenz) as little more than a highly addictive anti-retroviral (ARV) placebo that, when interrupted, produces withdrawal symptoms that AIDS clinicians routinely use to misdiagnose the onset of AIDS.
According to researchers, the following symptoms are known to be caused by HIV, AIDS, or drug withdrawal syndrome: - Fever (hyperpyrexia)
- Soaking night sweats
- Shaking chills or fever higher than 100 F for several weeks
- Headache
- Sore throat
- Cough and shortness of breath
- Skin rashes or bumps
- Chronic diarrhea
- Weight loss
- Persistent, unexplained fatigue
- Blurred and distorted vision
Drug Pushers Threaten Patients
When HIV clinicians identify these signs, they typically inform patients that the symptoms are directly “related to the onset of AIDS.” Some clinicians get angry, warning that unless they resume treatment of Sustiva drugs (like Atripla) “they will be dead within months.” When terrified patients resume their addiction, the symptoms subside – leading many to believe that the drug is staving off the effects of AIDS rather than perpetuating a physician-caused addiction.
Although OMSJ was on to the Sustiva scam last year, our researchers did not recognize the active components until this week when they discovered that a variety of benzodiazepine antibodies react with the Sustiva metabolite 8-hydroxy efavirenz.
OMSJ determined that use and withdrawal from addictive drugs like cocaine, alcohol, heroin, tobacco THC and benzodiazepine all suppress immune function.

Daniel Kuritzkes MD
Because smokers, alcoholics and junkies understand the lifesaving properties of a cigarette, martini or cough syrup after a week of abstinence, it’s hard to imagine how Harvard Professor Daniel Kuritzkes MD “didn’t know” that Bristol-Myers Squibb (BMS) scientists manipulated benzodiazepine in HIV drugs for the same reasons that Big Tobacco scientists manipulate nicotine levels in cigarettes. And while the Justice Department lists marijuana and benzodiazepine as controlled substances, Sustiva isn’t listed.
There’s more.
Years before Bristol-Myers Squibb (BMS) began pushing Sustiva (Efavirenz) in 1998, studies showed that benzodiazepines (BDZ) compromised immune function in sheep (1982) and mice (1988). In 1987, Arora (et al) found that a single dose of what they called “benzodiazepine receptor inverse agonists” caused “ a profound suppression of the immune response” in humans.
By 1992, Taupin (et al) found that a single injection of BDZ “markedly altered” immune function. Ferrarese (1992) and Zavala (1997) also linked BDZ to stress, anxiety and suppressed immune function.
One clue came in 2006, when researchers discovered that Sustiva produced urine samples that screen positive for marijuana and hashish (THC – see Blank, Roder and Rossi). Kuritzkes and BMS failed to disclose the highly addictive and psychotropic properties of Sustiva, marketing the poison as an ARV. They knew, or should have known, how Benzodiazepine receptors (GABAA) interact with Sustiva (8-hydroxy efavirenz) and how Sustiva causes effects very similar to benzodiazepines like Xanax, Rohypnol and DMCM.
Although BMS marketers may attribute this to “Sustiva inhibiting cytochrome P450 enzymes that metabolize the benzodiazepines,” the 8-hydroxy metabolite acts like a benzodiazepine. And like Big Tobacco’s manipulation of nicotine levels, benzodiazepines would dramatically increase Sustiva’s effect and toxicity.
Although Etifoxine (benzoxizone or BZX) is structurally different from benzodiazepines (BDZ), BZX binds to the same receptor site (GABAA) that binds with BDZ; producing many of the same highly addictive psychotropic reactions produced by BDZ. By using BZX as the active ingredient in HIV drugs, pharmaceutical companies are able to market a drug that delivers all of the highly addictive immune-compromising reactions without the use of BDZ. That, of course would be illegal and inconsistent with medical “standards of care.” But doctors who wouldn’t prescribe BDZ freely prescribe BZX.
Sustiva, T-cells and Immune Function
BMS pushed Sustiva as an HIV drug that lowers viral loads and increases T-cell counts, researchers attribute these changes to the redistribution of CD4 T-cells from lymphoid tissues during the first few weeks of drug use (see also Pakker, Andersson and Hazenberg). These papers show anti-HIV drugs do not increase the production of CD4 by suppressing HIV but by changing the relative amounts of T-cells in lymphatic tissue and blood.
Consider this analogy: In peacetime most soldiers are located within military bases and not throughout the general population. But when a disaster occurs, soldiers leave the bases and swarm towards attacked sites. While the absolute number of soldiers has not changed, where you find them has.
HAART treatment causes CD4 cells residing in lymphatic tissue to be released into the blood. That’s why the number of CD4 cells, as well as most other immune cells, increases after taking the drugs. This is a non-specific toxic effect of the drugs. The same thing occurs during chemotherapy for cancer.
A similar but opposite effect of HAART is its inhibition of the production of mRNA (messenger RNA). This explains the reduction in RNA “viral load” results after a person takes HAART (see Bucy & Andersson).
Sound far-fetched?
While OMSJ found no “smoking gun” related to the deliberate manufacture and sale of highly addictive psychotropic drugs under the pretext of HIV medication, the fact that the pharmaceutical industry has paid $8 billion (since 2004) to settle thousands of criminal and civil complaints related to the illegal marketing of drugs that cause thousands of preventable injuries and deaths suggests otherwise. Heavily distributed in Africa, the taxpayer-funded drug is a win for both junkies who smoke it like crystal meth and AIDS scientists whose research is funded by clinicians who identify the drug symptoms as AIDS.
When companies like Pfizer, GSK and Astra Zeneca illegally push drugs that generate $Billions annually, a few million-dollar fines become nothing more than “business expenses” that are routinely passed along to taxpayers and insurance companies.
This may also explain why Kuritzkes and his cohorts became unhinged after the release of House of Numbers (2008).
.
|
|
|
| 1 user liked this post |
|
02-04-2012, 11:22 PM
|
#202
|
|
Valued Poster
Join Date: Nov 7, 2010
Location: Top of The World
Posts: 601
|
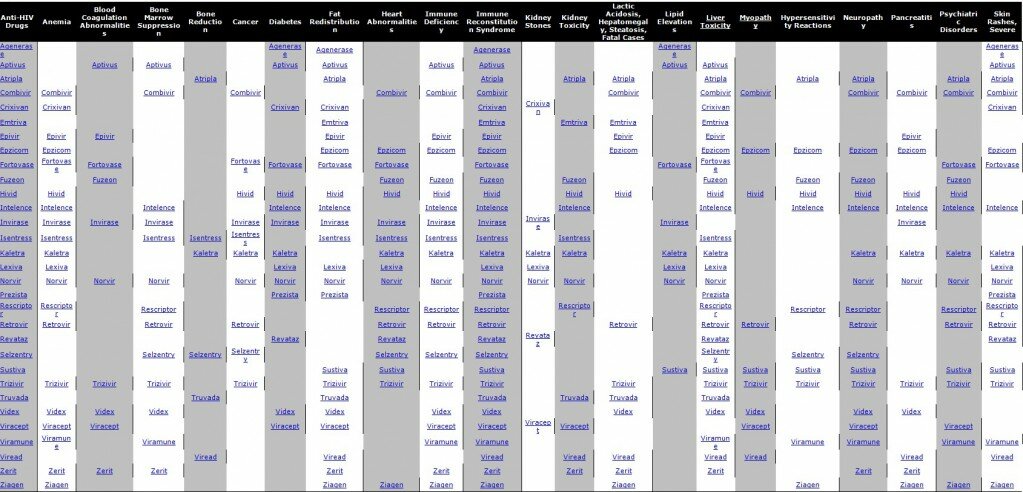
HIV Drug-Disease Matrix
Several years ago, graduate students at MITs PDOS research group attended the 9th World Multi-Conference of Systemics, Cybernetics, and Informatics. Although their research paper Rooter: A Methodology for the Typical Unification of Access Points and Redundancy was accepted,
their submission was nothing more than a randomly generated set of incomprehensible words organized to sound like legitimate science to challenge low submission standards for academic content. (Readers can generate their own scientific papers here.)
Although their harmless prank exposed scientific corruption, the pharmaceutical industry routinely produces similar gibberish to confuse their audience. Like the 19th century salesmen who rode into town hawking cocaine and opiates as elixirs, their pharmaceutical progeny continues to market disease and deadly or highly addictive cures that kill or injure millions of Americans every year.
Since infectious disease became statistically insignificant by 1955, the NIH and CDC have wasted billions of tax dollars convincing Americans that theyll die without medications that cause disease and kill.
But how are we supposed to know? Whether we read this advertisement or label information, we end up trusting clinicians who are paid to push drugs that kill.
GlaxoSmithKline: Zidovudine has been associated with hematologic toxicity including neutropenia, anemia
Prolonged use has been associated with symptomatic myopathy
Lactic acidosis and severe hepatomegaly with steatosis, including fatal cases, have been reported with the use of nucleoside analogues
Suspend treatment if clinical or laboratory findings suggestive of lactic acidosis or pronounced hepatotoxicity occur
That doesnt sound too bad, but what does it mean? Plain English:
Zidovudine (and other AIDS drugs) causes liver, kidney and immune diseases. Healthy and unhealthy people who take HIV drugs will eventually acquire cancer or an immune deficiency syndrome that will sicken or kill them. All 4 classes of antiretrovirals (ARVs) and all 19 Food and Drug Administrationapproved ARVs have been directly or indirectly associated with life-threatening events and death. (Reisler et al, 2003).
Virological response after starting HAART improved over calendar years, but such improvement has not translated into a decrease in mortality. (Lancet 2006)
OMSJs (Plain-English) HIV Drug Guide
To make sense of HIV drugs and packaging material, OMSJ has produced this guide that translates packaging material into easily understood warnings. If you take HIV drugs now, click on drugs and the diseases they cause. If you dont see a drug, contact OMSJ and well add it.
.
|
|
|
| 1 user liked this post |
|
02-04-2012, 11:36 PM
|
#203
|
|
Valued Poster
Join Date: Nov 7, 2010
Location: Top of The World
Posts: 601
|
In Defense of AIDS Critics
Profits of the AIDS industry run into many billions of dollars every year. When AIDS dissidents speak up, they are ridiculed with often ad hominem arguments. Here, the AIDS dissident John Lauritsen looks at one piece of ridicule in particular, and questions why he was not allowed to write a reasoned reply in a British humanist publication.
According to the German philosopher, Arthur Schopenhauer (17881860), All truth passes through three stages: first, it is ridiculed; second, it is violently opposed; third, it is accepted as being self-evident. Id add that, even before ridicule, truth will be ignored or censored, especially if powerful political-economic interests are involved. There is a German word for this: Todschweigen (to kill off through silence).
For over a quarter of a century there have been critics of the orthodox AIDS paradigm, the HIV-causes-AIDS hypothesis. We call ourselves AIDS dissidents or AIDS critics or AIDS realists. We have experienced every imaginable form of censorship and ridicule, and now, as our ranks have grown, violent opposition, which almost always attacks our persons, not our ideas.
Dr Mark Wainberg, president of the International AIDS Society, has called for jailing AIDS dissidents, whom he calls HIV deniers (his explicit analogy to Holocaust deniers). John P Moore of Cornell University advocates even more violent measures, stating, This is a war, there are no rules, and we will crush you, one at a time, completely and utterly (at least the more influential ones; foot-soldiers like you arent worth bothering with). (Letter from John P Moore, PhD to AIDS dissident Michael Geiger, 27 Jan. 2007.)

John P. Moore PhD:
This is a war, there are
no rules, and we will crush
you, one at a time,
completely and utterly..."
The latest attack pit bull for the AIDS Establishment is Seth Kalichman, a clinical psychologist, who has written several books on AIDS and set up his own blog ( see Related links, below). An article by Kalichman Are You Positive? Rogues, pseudoscientists, snake oil peddlers appears in the November/December 2009 issue of the British publication New Humanist. Kalichman goes for the jugular, portraying us as warped, devious, evil people. According to him, we are responsible for untold deaths of those who, following our ideas, avoid anti-HIV drugs. Kalichmans article has a sidebar, taking up two-thirds of a page The Denialist Hall of Shame which gives headshot photos and derisively untrue descriptions of Peter H Duesberg, David Rasnick, Jody Wells, Huw Christie, Michael Baumgartner, Neville Hodgkinson, Gordon Stewart, the Perth Group (Eleni Papadopulos-Eleopulos and Valendar Turner), Henry H Bauer, Christine Maggiore, David Crowe, and Kary B Mullis. (I, to my regret, am omitted.)
AIDS cash cow
Before going into the specifics of Kalichmans article, I must defend the good names of AIDS dissidents. We are not bad people, who in some sinister (if unspecified) way are profiting from the stands we have taken. This is the opposite of the truth. Believe me, there are no financial rewards for attacking the AIDS cash cow. The AIDS dissidents I know have been motivated by a concern for truth and a desire to save lives. All of us have taken hard knocks; all have suffered social, professional and financial losses. AIDS dissidents have been ostracised and slandered; fired or had grants cancelled; driven into bankruptcy; physically assaulted.
Profits of the AIDS Industry run into many billions of dollars every year. This is where the money is. People with meagre qualifications have become rich as AIDS experts, heads of AIDS organisations, or treatment activists. Regardless of how Wainberg, Moore and Kalichman receive their compensations, there can be no doubt that their interests lie with Big Pharma. The crux of the matter is revealed in Kalichmans panegyric to HIV treatments: People are living longer and healthier lives with HIV infection as a result of earlier detection through HIV antibody testing and a remarkable success of HIV treatments. Indeed, countries that launched aggressive testing and treatment programs, such as Brazil and Botswana, have reduced suffering and prolonged life. In contrast, South Africa delayed testing and treatment programs as a result of former President Thabo Mbekis AIDS denialism, policies that resulted in over 300,000 unnecessary deaths and over 35,000 infants senselessly infected with HIV.
There is not a word of truth in this. The HIV-antibody tests have never been validated, so no one knows exactly what they mean, let alone how reliable they are. A German AIDS dissident, Erhard Neubert, said it exactly: The virus doesnt kill, the diagnosis does. Healthy people who receive HIV-positive diagnoses are prescribed drugs that cause malaise, deformity and eventually death. Many deaths among HIV-positive people now occur from liver cancer or other forms of organ failure caused by HIV treatments. Since many of these HIV-positives never acquire an AIDS-indicator condition, they are not counted as AIDS deaths, thus perpetuating the myth that AIDS deaths are dropping thanks to anti-HIV drugs. The reality is that HIV treatments are killing people who were healthy before taking them1.
So far as South Africa is concerned, the figures are made up from whole cloth. AZT,* the drug Big Pharma was marketing to Africa, would not have saved lives, but destroyed them. AZT is a drug on which I have written extensively. Using documents obtained from the US Food and Drug Administration under the Freedom of Information Act, I demonstrated that AZT was approved on the basis of fraudulent research ( see FDA Documents Show Fraud in AZT Trials on the VirusMyth website). AZT is cytotoxic, meaning that it harms healthy cells. The toxicities of AZT include anaemia, myopathy (muscular pain, muscular inflammation, muscular atrophy), cachexia (wasting), nausea, headache and damage to the kidneys, liver and nerves.

Seth Kalichman PhD received
$17 million to blog for AIDS Inc.
AZT is a known carcinogen. (It is highly positive in a standard test for carcinogenicity, the Cell Transformation Assay; it causes cancer in rodents; and there is a strong correlation between long-term AZT therapy and cancer of the lymph system.) AZT is a random terminator of DNA synthesis, the very life process, without which body cells can neither be formed nor develop.
In the United States alone, upwards of a third of a million gay men have been murdered through AZT. I say murdered, because the drug was criminally approved for marketing on the basis of fraudulent research, and because it was promoted through fraudulent claims that the HIV-positives would have better and longer lives. Most of these gay men would be alive today if they had avoided AZT and had taken appropriate health measures for example, giving up cigarettes and drugs (including poppers).
Kalichmans article, as well as his book, Denying AIDS (2009), consists of nothing but ad hominem argumentation attacking the persons, but not the ideas, of AIDS critics. Indeed, he explicitly states that he will not enter into scientific debate: This is not a book about AIDS and how it is caused by HIV. Rather, this is a book about HIV/AIDS denialism. I did not write this book to answer the denialist claims, but rather to offer insight into their wacky and destructive world [Denying AIDS, p. xv].
Kalichman urges us to trust true experts and scientists who know more than we do to decipher the technical details ( Denying AIDS, p. 156). Using a variant of the tired old argument, Eighty million Frenchmen cant be wrong, he writes: Tens of thousands of studies show that HIV does cause AIDS. If HIV does not cause AIDS it would mean that thousands of scientists, researchers, medical doctors, and public health officials essentially the entire biomedical science and public health enterprise had conspired to maintain a lie for 25 years [p. 111].
Kalichman portrays HIV/AIDS denialists as mentally ill individuals, filled with suspicion and paranoia, who are obsessed with other kinds of denialism and conspiracy theories. In his book he refers to those who doubt that the Holocaust or 9/11 ever happened (p. 9) a strange statement. Thousands of people including top-notch architects, physicists and engineers dispute the governments explanation of why three buildings (WTC1, WTC2 and WTC7) collapsed in the way that they did, but none have denied that the buildings collapsed, or that two of the three buildings were hit by aeroplanes.
Conspiracies do exist
Of course, conspiracies do exist. In business or in politics, they are part of the game. While denying the conspiracies in which we AIDS critics allegedly believe, Kalichman seems to believe that we ourselves form some sort of conspiracy. Using stealth tactics and the pseudonym of Joseph (Joe) C Newton to penetrate our ranks, he ingratiated himself with some of us (not me), professing to greatly admire our work. This was pointless, as we have nothing to hide and our ideas are readily available. Kalichman seems particularly proud of his incognito relationship with Peter Duesberg: on Page 27 of his book is a photo of himself next to Duesberg.
The ugliest ad hominem tactic used by Kalichman and others of his ilk is to gloat over the deaths of a few AIDS dissidents, arguing speciously that their deaths were caused by HIV, and they would have lived longer had they taken anti-HIV drugs. Without going into personal details, I can say that in every case there were health risks in their lives, having nothing to do with viruses, which could explain why they died.
What about the hundreds of thousands of people, in the United States alone, who died while taking anti-HIV drugs? Did the drugs kill them? What about the prominent advocates of AZT therapy who have died in the past two decades? Did guilt cause them to develop cancer or succumb to organ failure? Consider the recent death of Stephen Lagakos, who co-authored a bogus study (Paul Volberding, Stephen Lagakos et al., New England Journal of Medicine, 5 April 1990), which advocated giving AZT to asymptomatic HIV-positives. Driving on the highway in October 2009, Lagakos suddenly veered over into the lane of oncoming traffic, killing himself, his mother, his wife and the man in the other car. Was Lagakos killed by an Avenging Conscience? Why not? The conjecture is, if anything, just as rational as the conjecture that AIDS-dissidents were killed by a retrovirus.
In an earlier book, Understanding AIDS: Advances in Research and Treatment (1998), Kalichman toes the line of AIDS orthodoxy, and doesnt even mention AIDS critics. In addition to the usual AIDS commodities, Kalichman puts in a pitch for those of the Therapy Industry. Kalichmans fellow psychologists have observed that gay men with AIDS diagnoses suffer from depression. Why? A rationalist might say that gay men are depressed because, for over two millennia, the Abrahamic religions (starting with the Holiness Code of Leviticus) have punished sex between males with death; because religionists, from the Catholic church to the Moral Majority to the Rev. Fred Phelps, have told gay men that they are going to Hell and should die; because Hollywood movies have conveyed the message that gay men should commit suicide, be murdered or both; because gay men with HIV-positive diagnoses have been told that they have a fatal disease; because they have been prescribed anti-HIV drugs, which make them feel awful and cause physical deformities (Crix bellies, buffalo humps, bulging veins in the head, shrivelled arms and legs, wasted deaths-head faces, greyish or cyanotic skin colour). Anyone with eyes open can see that gay men, with or without HIV-positive diagnoses, have ample reasons to be unhappy.
But Kalichman, ignoring all of these reasons, argues that gay men with AIDS diagnoses need therapy, as well as anti-depressant drugs drugs that cause irreversible neurological damage, and that have caused previously sensible people to commit murder and/or suicide. In thus blaming the victim, Kalichman follows in the footsteps of an earlier shrink, Irving Bieber, who in the 1950s sneeringly diagnosed gay men as injustice collectors (as though we were not the victims of real injustices).
Debate denied
Kalichman, both in his New Humanist article and in his books, does not want his readers to know the real arguments of AIDS critics or where to find them. Notably missing are references to our books or URLs to our websites. In Denying AIDS, one paragraph in Appendix B (about the HIV/AIDS Denialists) mentions me and gives a brief quote from my book, The AIDS War an atypical quote torn out of context. There is a superscript number, but no note, so the reader would have no idea where the quote came from. Indeed, there are no endnotes at all for Appendix B, although there are 14 superscript numbers, one more example of the sloppiness of this shoddy little book. When ad hominym appears for ad hominem the reader suspects that Kalichman doesnt understand the concept any more than the spelling.
It is regrettable that Kalichmans stridently abusive article should have appeared in the New Humanist, which was once a distinguished publication. I subscribed to the New Humanist for many years, until about 2002, when the layout became uglier and less readable, and the content became increasingly alien to freethought or humanism.
As soon as I became aware of Kalichmans article, I wrote Editor Caspar Melville in March this year, asking if I could write a rebuttal piece. He replied: I appreciate your offer but in this instance I dont think there is a case for publishing a rebuttal. When we published Kalichmans piece we got quite a lot of comment from the dissidents on our blog, (most of which Im afraid to say seemed to confirm his argument) [see here].
So I feel that we have covered the issue well, allowed space for rebuttal, and there is little point in going over it again.
I replied: You are the editor, so thats that. Of course I dont agree with your decision. Blogs open to anyone and everyone are hardly a substitute for a rebuttal in the same publication as the piece being rebutted. Its elementary fair play that a rebuttal should be written by someone qualified to make the case for the opposing viewpoint.
The New Humanist blog didnt allow much space for rebuttal, since it was closed after AIDS dissidents entered the discussion. Melville chose not to suggest that I write a letter to the editor, so even that small space for rebuttal was not open. This is a shame, because in the past Melville seemed to favour open and vigorous debate over controversial issues. In his first editorial he wrote, Humanists are sceptics. Above all, they believe in doubt ( New Humanist, September/October 2005). In a later editorial he wrote: While both [Richard] Dawkins and [Christopher] Hitchens are polemicists whose aim is to challenge, stimulate and infuriate they do also make strong and serious arguments which should be engaged at the level of logic and reason. Are they wrong? If they are, where are the counter-arguments beyond calling them names, or equating them with book-burners and murderers? [New Humanist, March/April 2007.]
We AIDS critics have also put forward strong and serious arguments, which have so far not been engaged at the level of logic and reason. We do not deserve to be called rogues, pseudoscientists, snake oil peddlers.
On every front cover of New Humanist is stated, A magazine for freethinkers. That may once have been so, but it is now false advertising.
1 United States deaths of people with AIDS diagnoses
.
|
|
|
| 1 user liked this post |
|
02-04-2012, 11:37 PM
|
#204
|
|
Account Disabled
Join Date: Jan 24, 2010
Posts: 3,039
|
Worthy messages, screwed up by unhinged individual?????
|
|
|
| 1 user liked this post |
|
02-05-2012, 12:05 AM
|
#205
|
|
Valued Poster
Join Date: Nov 7, 2010
Location: Top of The World
Posts: 601
|
BIIDS: Behavioural Induced Immune Deficiency Syndrome
Johnson Tagarisa grew up during the 1970s when his cousins, brothers and uncles worked in the mines of South Africa. Upon return to their native Zimbabwe, they spoke often of their experiences. By the time that people were starting to “die from AIDS in South Africa,” Johnson was old enough and educated enough to connect the dots. Even when his stepbrother died in 1993, Johnson argued with the doctor that he had died of syphilis because he had every symptom of advanced syphilis.
Johnson studied economics and finance at the University of Toledo Ohio and is an avid follower of statistics in many subject areas – including HIV.
by JOHNSON TAGARISA
BSC, MA MBA
The model of Behaviour Induced Immune Deficiency syndrome (BIIDS) in America takes the form of drug abuse and extreme experimentation with drugs in the Gay and Lesbian communities. In Southern Africa it came with the “Blessings” of WENELA. (Witwatersrand Native Labour Association). WENELA was the organ responsible for recruiting labour for the South African mines. It represented shrewd and oppressive labour contracts drafted between the host country – Apartheid South Africa and supply countries of Southern, East and central Africa. At its peak WENELA drew hundreds of thousands, if not millions (cumulatively), of young men migrant labourers to the mines. The main catchment area for WENELA were the southern African countries of Mozambique, Lesotho, Swaziland, Zimbabwe, Zambia, Botswana, Malawi, Namibia, Zaire and as far afield as Tanzania.
Colonial Origins
Colonial Southern Africa was a place like any other, where European conquest meant the natives became second class citizens, denied of equal opportunity in employment and any other social amenities that came with modernity. The only job opportunities accorded to black natives, at professional level, were such jobs as teaching and nursing, a few services and if only they could give those services in their communities. Townships sprung up through out Sub-Saharan Africa in the 20th century. These were basically Ghettos characterized by over-crowdedness, continued neglect and filth, to say the least. Continued migration from the country to the city continues up to today in many African Countries, but the current model of migration differs slightly from the earlier on model of migration.
In the early days, the migrants were mainly young men who came to the cities to seek employment and those married or otherwise left their loved ones back in the country. This happened mainly because of two reasons – migrating to the city did not guarantee good accommodation for the woman and the offspring. Secondly the municipalities had devised a system that made it unattractive for young men to make the cities their home. Accommodation that was provided by the Municipalities were the infamous Hostels. The Hostels were dormitories – single rooms in high rise buildings, 7m by 4m, for male migrant labourers. Typically designed to be shared by two people, the rooms ended up carrying as many as six people. No women were allowed in these single-sex hostels. The men who shared these hotels shared a communal toilet (Bathroom). Typically these places got overcrowded to the extend of there being one toilet for over 200 men per floor.

Two economic powerhouses of the colonial era were Rhodesia (Zimbabwe) and South Africa. With the advent of liberation struggle in Zimbabwe in the 60s and 70s, South Africa became the biggest magnet for migrant labour. All these people would be accommodated in the infamous Hostels. This gave rise to the proliferation of the shabeens. Shabeens were the informal residential outlets of alcohol – since the blacks were not allowed to drink at designated places and at least to drink at all. The shabeens primarily supplied two things, apart from entertainment, alcohol and prostitutes. “The single-sex hostels that provided for housing, offered systematic denial of normal family life to migrant workers, encouraged prostitution, the spread of communicable diseases such as TB, and widespread breaking of families and crime.”**
Prostitutes were sneaked into hostels and because these miners had very little disposable income, stories of people sharing a prostitute were many. Rumours of homosexuality, men having sex with men, surfaced at large for the first time in societies that traditionally regarded homosexuality a taboo. Common sexually transmitted diseases thus made a foothold with gonorrhea being the most common and syphilis the salient killer. Medical services given to these people were basic at most necessary to keep them going but not at all exhaustive. For many of the young men, the “underground medical services” provided the means to a desperately needed end. The use and abuse of medicines was rampant with no one checking.
Common uneducated but dangerous beliefs emerged. It was wildly believed taking antibiotics before sex was assurance that one would not contract an std, or taking at least four tablets the following morning was another quick remedy. A common occurrence was taking the antibiotics at the shabeens – with a swallow of alcohol. The use and abuse of alcohol, marihuana and medical drugs was unprecedented while apartheid South Africa did not have a comprehensive and appropriate medical system to control and fight the diseases among mining communities. To supplement the medication was the practice of taking medical herbs which saw traditional herbalists make brisk business from diseases that were traditionally not part of their culture. My personal observations, with most of the medical herbs is that, they fail to do much in clearing the bacterium such as gonorrhea let alone syphilis. For one, while some medication was available for other sexually transmitted diseases the deadly syphilis was inadequately tested or treated, it remained deliberately under-detected and under-treated.

Mining Diamonds in South Africa
By the time the WENELA program died down, a lot of medically resisting bacteria existed as parasites in the majority of these young men. The majority of these people left for home carrying their goodies and other “special” tiny presents with them. Men complained of an untreatable penal discharge that they used to see every morning when they woke up. They went back to Lesotho, Swaziland, Botswana, Zimbabwe, Malawi, Mozambique and other sub-Saharan African countries. At a time when most of these young men started dying in the late eighties, emphasis was on the new scourge AIDS even when most of the symptoms were very similar to syphilis, the AIDS stigma gripped many nations, people panicked and common sense was completely lost in the medical field. (Most of the people who have died from the so called AIDS, are people born between 1945 and 1969 and those who might have contracted the BIIDS bugs and never got adequate and appropriate treatment.). The fact that in SA the “disease” has killed more black people than white people (in percentage terms) would be better be explained by the former Minister of Health of Apartheid South Africa, if the majority of us are too dump to put the dots together.
Compounding the death scourge was the fact that, in the sixties and seventies, southern Africa was involved in wars of liberation struggle. At its peak Rhodesia (Zimbabwe) had concentration camps where people would never be immunized against common diseases. Political stability did not correspond to health stability in Southern Africa. All those young men and people who had been displaced by either labour Migration (WENELA) or War did not get immunized nor did they get tested for syphilis. It is always a common trend in post war African nations. Those raped during the struggle will never receive proper counseling let alone proper medical diagnosis and treatment. The United Nations facilitates relocation without rehabilitation – thanks a lot to them. (Just wait and watch the Dafur crisis – when it is over, all the children who missed immunizations will never be immunized and all the women who were raped will never be checked, tested and treated for communicable Stds and TB, but overfunded HIV researchers will be the first to find experimental “monkeys” among these people– just watch and see. It is always the poor, illiterate and desperate who are easier to manipulate).

Secondary syphillis
The underground system of medication continued for a very long time in these countries – and as we speak, syphilis is not a reportable disease in Southern and Central Africa and is hardly tested. Genital herpes is basically ignored. One can be treated of gonorrhea five times a year, using the standard antibiotic prescription, and the medical doctor would never sagest that this person be tested for other diseases, like syphilis or perhaps change his medication to a stronger penicillin injection that could knock off the resistant gonorrhea.
“The mining sector in particular has a stubbornly high rate of disablement and deaths. The inability of the current and previous systems at the mines to prevent, gauge, and adequately compensate for occupational injury and illness, to include associated social illnesses related to social and cultural disruption, poor health provision is well recognized. The legacy of under-recognition and under-detection of occupational illnesses persisted into the 1990s. This is compounded by the fact that ill-health may only emerge some time after employment when the migrant has returned home. Time lags of up to 20 years between exposure to risk factors on mines and detectable diseases to mine workers (and those they probably infected) place the burden of ill-health on the supplying country. In case of sickness, injury and disability, migrants fall back on rural households and poorly equipped and failing public health systems of home countries” – in short, these sick and exhausted labourers go back home to die.
Parallels are drawn to the Tuskegee experiment of USA. The experiment involved a group of 399 black men used as “monkeys” in a medical research for a forty year period, 1932 to 1972. The men had latent syphilis a disease that was prevalent during the era. The standard treatments available at that time were known to be highly toxic and there were grave doubts about their effectiveness. This selected group of men was not showing symptoms at that time. Even after 1947 when an effective antibiotic treatment became available these men were deliberately denied treatment and they were thus left to degenerate in response to the ravages of tertiary syphilis – which includes tumors, heart disease, blindness, paralysis, insanity, and death. ( someone remember the descriptions of the illness symptoms and deaths associated with AIDS on the onset of the “discovery” of the disease?). As the degeneration progressed and a significant number died, the CDC of America collected the data.
The data which they did not collect was my major concern, when I first saw a documentary and a film about the story. They did not collect data about how many more people were infected by these “monkeys” before they died. Two hundred and fifty of the group were served by the bell. They joined the US army on the onset of WWII where they were ordered to be treated for syphilis. And as I write, it is my big suspicion that many people of African American communities are still dying from the ripple effect of the Tuskegee experiment, for up to now, there has not been a comprehensive program set by the American Government to curb the ripple effects of the experiment – (well it is affecting mostly black people, and those whites now allowed to sleep with black people). You could have thought a country as big and as rich as America would have a compensatory program that encourages sexually active Blacks to be tested for syphilis, once in every two years free of charge. Then if they are found to be infected with the syphilis pathogen they get free treatment. This would be the best compensation for these descendants of slaves, the majority who remain socially oppressed and languishing in poverty, and thus resorting to prostitution and drugs for survival. – but alas wisdom died long ago with Socrates before America was “discovered”. As logic would dictate, first things first – attack the devil you know. All the money used to fund AIDS programs could be used to curb social ills and correct the syphilis situation in USA.
Conclusion
One thing that often irritated me when I entered higher learning was a topic question that required me to self critique – that is to criticize my own findings or my own proposals. The worst irritation came when my best friends made “ground beef” of my presentation in front of a professor. I soon realized and accepted, though, that it was standard practice in higher learning to present your work for criticism. That is the democracy in the academic and scientific world. What worries me today is the lack of such democracy when it comes to issues regarding HIV/AIDS research. From the time of Gallo’s “discovery” to this day, none of the AIDS theories is questioned or criticized before publication – everything is given as fact and the public has to take it.
While I do not want to challenge the existence of a virus dubbed HIV, I would like to draw people’s attention to the correlation of immune deficiency in humans that is acquired through social ills or social behaviours. And in the name of academic democracy never to stop questioning and if any of the so called “experts” have defeated the known protocols of research and publication, the public has the right to know the truth and, just as no one is above the law in society – no one is above academic scrutiny in matters that affect the world at large. Robert Gallo’s paper must be challenged.
** Refs : Quotations from “ African Migrant Labour Situation In Southern Africa” – by Dr Godfrey Kanyenze – March 2004 ( italics mine.)
Johnson Tagarisa currently resides in Toronto, Ontario.
.
|
|
|
| 1 user liked this post |
|
02-05-2012, 12:14 AM
|
#206
|
|
Account Disabled
User ID: 106202
Join Date: Oct 24, 2011
Location: Dallas
Posts: 50
My ECCIE Reviews
|
I admit, i'm going to have to read this book in its entirety. I will, however, always play safe.
|
|
|
| 1 user liked this post |
|
02-05-2012, 12:40 AM
|
#207
|
|
Valerie's Mod Husband
Join Date: Dec 13, 2010
Location: Houston
Posts: 28,030
|
Quote:
Originally Posted by Mr. Bill
Why? ...because it appeared no one else had the essential competency, a selfless inclination, or the balls to speak up.
|
You're constantly missing the question. I'm not asking why you posted this topic. I'm not interested in your state of mind or the state of your balls. I'm interested in why you picked this site to post it to.
|
|
|
| 1 user liked this post |
|
02-05-2012, 12:45 AM
|
#208
|
|
Valued Poster
Join Date: Nov 7, 2010
Location: Top of The World
Posts: 601
|
Quote:
Originally Posted by desi.snakes
I admit, i'm going to have to read this book in its entirety. I will, however, always play safe.
|
Thank you for your comments Desi.
.
|
|
|
| 1 user liked this post |
|
02-05-2012, 12:50 AM
|
#209
|
|
Valued Poster
Join Date: Nov 7, 2010
Location: Top of The World
Posts: 601
|
Quote:
Originally Posted by Wakeuр
You're constantly missing the question. I'm not asking why you posted this topic. I'm not interested in your state of mind or the state of your balls. I'm interested in why you picked this site to post it to.
|
I tire of your questions ...draw your own conclusions ...you'll do that anyway ...regardless of my answers.
.
|
|
|
| 1 user liked this post |
|
02-05-2012, 01:08 AM
|
#210
|
|
Account Disabled
User ID: 106202
Join Date: Oct 24, 2011
Location: Dallas
Posts: 50
My ECCIE Reviews
|
I believe I may understand why he posted on this site. It makes sense to me. For one, we are possibly the most open-minded group of people in terms of debating such a hot topic. We are also some of the most professionally diverse, therefore more willing to acknowledge discrepancies in estimations, summations, and faulty research. We are all very aware of the realization of STD's in this community. He's not negating the existence of HIV/AIDs, merely bringing to light some very concerning issues regarding the discovery, development, and treatment of the virus. I suppose it helps that I have a background in science and chemistry. It's a tough read, but I did enjoy the comparison between the Tuskegee Experiments and the parallels between Syphilis and AIDs. I must say, that was some of the best reading i've experienced in quite a while. I, for one, thank you for bringing forward this debate.
|
|
|
| 1 user liked this post |
|
|
AMPReviews.net |
|
Find Ladies |
|
Hot Women |
|